
Nutrition Meets Social Marketing: Targeting Health Promotion Campaigns to Young Adults Using the Living and Eating for Health Segments

 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Market Segmentation
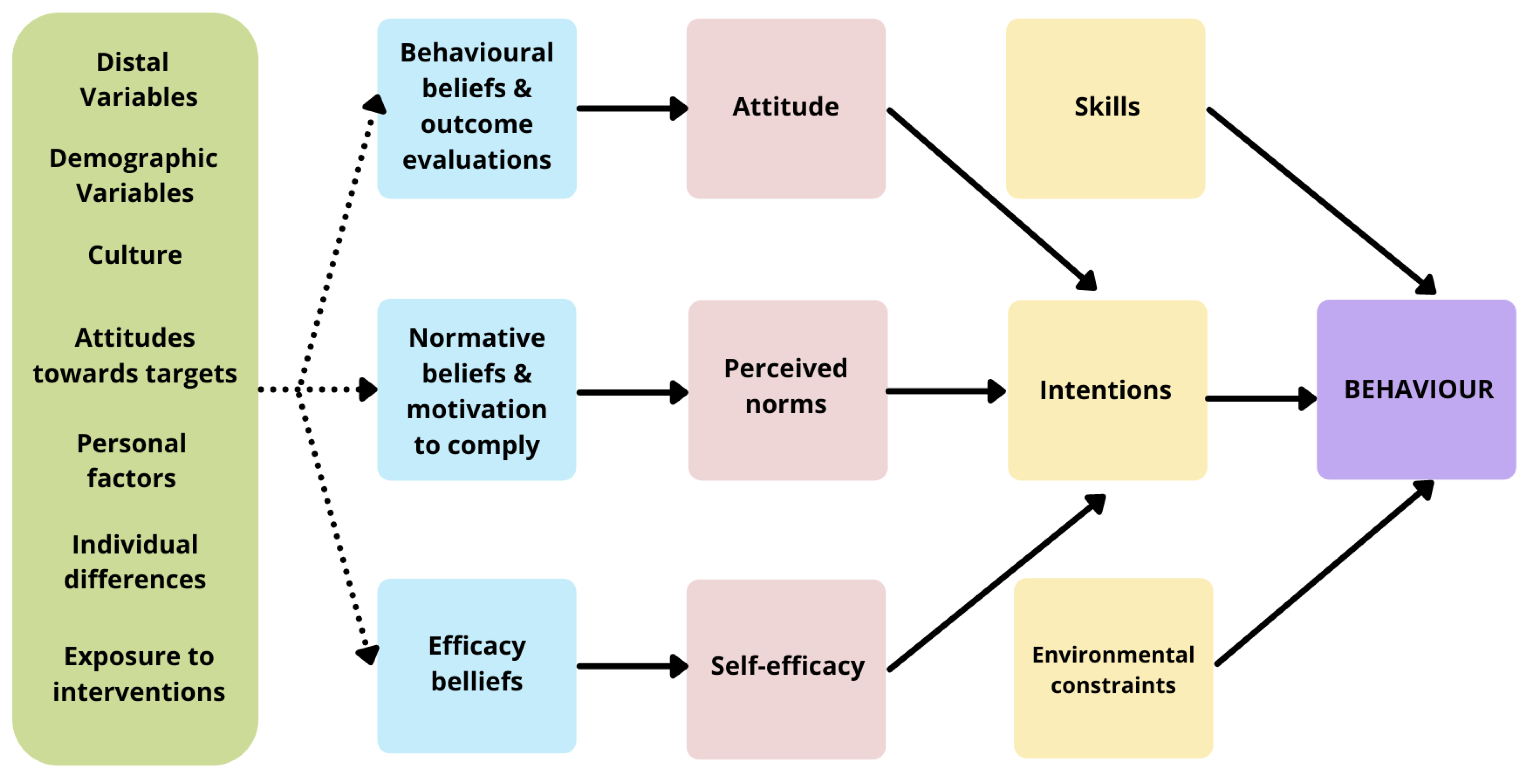
1.2. Theoretical Framework
2. Materials and Methods
2.1. LEHS Development
2.1.1. Literature Reviews
2.1.2. Qualitative Research
2.1.3. Quantitative Survey
- Lifestyle Mavens: I am passionate about healthy eating and health plays a big part in my life. I use social media to follow active lifestyle personalities or get new recipes/exercise ideas. I may even buy superfoods or follow a particular type of diet. I like to think I am super healthy.
- Health Conscious: I am health-conscious and being healthy and eating healthy is important to me. Although health means different things to different people, I make conscious lifestyle decisions about eating based on what I believe healthy means. I look for new recipes and healthy eating information on social media.
- Aspirational Healthy Eaters: I aspire to be healthy (but struggle sometimes). Healthy eating is hard work! I have tried to improve my diet, but always find things that make it difficult to stick with the changes. Sometimes I notice recipe ideas or healthy eating hacks, and if it seems easy enough, I will give it a go.
- Balanced All Rounders: I try and live a balanced lifestyle, and I think that all foods are okay in moderation. I should not have to feel guilty about eating a piece of cake now and again. I get all sorts of inspiration from social media like finding out about new restaurants, fun recipes, and sometimes healthy eating tips.
- Contemplating Another Day: I am contemplating healthy eating but it is not a priority for me right now. I know the basics about what it means to be healthy, but it does not seem relevant to me right now. I have taken a few steps to be healthier, but I am not motivated to make it a high priority because I have too many other things going on in my life.
- Blissfully Unconcerned: I am not bothered about healthy eating. I do not really see the point and I do not think about it. I do not really notice healthy eating tips or recipes and I do not care what I eat.
2.2. Statisticial Analysis
3. Results
3.1. Behavioural Beliefs
3.2. Skills in Relation to Food and Food Preparation
3.3. Normative Beliefs and Motivation to Comply
3.4. Environmental Constraints
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Government. Selected Higher Education Statistics—2015 Student Data. In Department of Education and Training; Australian Government: Canberra, Austrlia, 2016. [Google Scholar]
- Ashton, L.M.; Hutchesson, M.J.; Rollo, M.E.; Morgan, P.J.; Collins, C.E. A scoping review of risk behaviour interventions in young men. BMC Public Health 2014, 14, 957. [Google Scholar] [CrossRef] [Green Version]
- Munt, A.E.; Partridge, S.R.; Allman-Farinelli, M. The barriers and enablers of healthy eating among young adults: A missing piece of the obesity puzzle: A scoping review: Barriers and enablers of healthy eating. Obes. Rev. 2017, 18, 1–17. [Google Scholar] [CrossRef]
- Bastien, M.; Poirier, P.; Lemieux, I.; Després, J.-P. Overview of Epidemiology and Contribution of Obesity to Cardiovascular Disease. Prog. Cardiovasc. Dis. 2014, 56, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Abate, N.; Chandalia, M. Role of subcutaneous adipose tissue in metabolic complications of obesity. Metab. Syndr. Relat. Disord. 2012, 10, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Apovian, C.M.; Gokce, N. Obesity and cardiovascular disease. Circulation 2012, 125, 1178–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia; National Health and Medical Research Council: Melbourne, Australia, 2013; p. 232.
- Black, N.; Hughes, R.; Jones, A.M. The health care costs of childhood obesity in Australia: An instrumental variables approach. Econ. Hum. Biol. 2018, 31, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finkelstein, E.A.; Graham, W.C.K.; Malhotra, R. Lifetime direct medical costs of childhood obesity. Pediatrics 2014, 133, 854–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, A.; Chevalier, A.; D’ Souza, M.; Baur, L.; Wen, L.M.; Simpson, J. Early childhood obesity: Association with healthcare expenditure in Australia. Obesity 2016, 24, 1752–1758. [Google Scholar] [CrossRef]
- Tsai, A.G.; Williamson, D.F.; Glick, H.A. Direct medical cost of overweight and obesity in the USA: A quantitative systematic review: USA obesity direct medical cost. Obes. Rev. 2011, 12, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescent Health 1 Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Molenaar, A.; Choi, T.S.T.; Brennan, L.; Reid, M.; Lim, M.S.C.; Truby, H.; McCaffrey, T.A. Language of health of young australian adults: A qualitative exploration of perceptions of health, wellbeing and health promotion via online conversations. Nutrients 2020, 12, 887. [Google Scholar] [CrossRef] [Green Version]
- Brennan, L.; Chin, S.; Molenaar, A.; Barklamb, A.M.; Lim, M.S.C.; Reid, M.; Truby, H.; Jenkins, E.L.; McCaffrey, T.A. Beyond body weight: Design and validation of psycho-behavioural living and eating for health segments (LEHS) profiles for social marketing. Nutrients 2020, 12, 2882. [Google Scholar] [CrossRef] [PubMed]
- Kitunen, A.; Rundle-Thiele, S.; Kadir, M.; Badejo, A.; Zdanowicz, G.; Price, M. Learning what our target audiences think and do: Extending segmentation to all four bases. BMC Public Health 2019, 19, 382. [Google Scholar] [CrossRef] [Green Version]
- Carins, J.E.; Rundle-Thiele, S.R. Eating for the better: A social marketing review (2000–2012). Public Health Nutr. 2014, 17, 1628–1639. [Google Scholar] [CrossRef] [Green Version]
- Snyder, L.B.; Hamilton, M.A.; Mitchell, E.W.; Kiwanuka-Tondo, J.; Fleming-Milici, F.; Proctor, D. A Meta-Analysis of the Effect of Mediated Health Communication Campaigns on Behavior Change in the United States. J. Health Commun. 2004, 9, 71–96. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, T.; Rundle-Thiele, S.; Kubacki, K. Segmentation in Social Marketing Process, Methods and Application, 1st ed.; Springer: Singapore, 2017. [Google Scholar]
- Dietrich, T.; Rundle-Thiele, S.; Schuster, L.; Drennan, J.; Russell-Bennett, R.; Leo, C.; Gullo, M.J.; Connor, J.P. Differential segmentation responses to an alcohol social marketing program. Addict. Behav. 2015, 49, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, E.L.; Legrand, S.; Brennan, L.; Molenaar, A.; Reid, M.; McCaffrey, T.A. Psycho-behavioural segmentation in food and nutrition: A systematic scoping review of the literature. Nutrients 2021, 13, 1795. [Google Scholar] [CrossRef]
- Lombard, C.; Brennan, L.; Reid, M.; Klassen, K.M.; Palermo, C.; Walker, T.; Lim, M.S.C.; Dean, M.; McCaffrey, T.A.; Truby, H. Communicating health-Optimising young adults’ engagement with health messages using social media: Study protocol: Communicating health study protocol. Nutr. Diet. 2018, 75, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Lotenberg, L.D.; Schechter, C.; Strand, J. Segmentation and targeting. In The SAGE Handbook of Social Marketing; SAGE Publications Ltd.: London, UK, 2011; pp. 125–135. [Google Scholar]
- French, J. The importance of segmentation in social marketing strategy. In Segmentation in Social Marketing; Springer: Singapore, 2017; pp. 25–40. [Google Scholar]
- Fishbein, M.; Yzer, M.C. Using Theory to Design Effective Health Behavior Interventions. Commun. Theory 2003, 13, 164–183. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Klassen, K.M.; Douglass, C.H.; Brennan, L.; Truby, H.; Lim, M.S.C. Social media use for nutrition outcomes in young adults: A mixed-methods systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 70. [Google Scholar] [CrossRef] [Green Version]
- Rounsefell, K.; Gibson, S.; McLean, S.; Blair, M.; Molenaar, A.; Brennan, L.; Truby, H.; McCaffrey, T.A. Social media, body image and food choices in healthy young adults: A mixed methods systematic review. Nutr. Diet. 2020, 77, 19–40. [Google Scholar] [CrossRef]
- Walker, T.; Palermo, C.; Klassen, K. Considering the impact of social media on contemporary improvement of Australian Aboriginal health: Scoping review. JMIR Public Health Surveill. 2019, 5, 64–71. [Google Scholar] [CrossRef]
- Brennan, L.; Voros, J.; Brady, E. Paradigms at play and implications for validity in social marketing research. J. Soc. Mark. 2011, 1, 100–119. [Google Scholar] [CrossRef]
- McCaffrey, T.; Brennan, L.; Reid, M.; Molenaar, A.; Chin, S. Survey—Living and Eating for Health Segments (LEHS) and Social Media Use: Implications for Improving Healthy Eating Practices. 2020. Available online: https://bridges.monash.edu/articles/workflow/Survey_-_Living_and_Eating_for_Health_Segments_LEHS_and_Social_Media_Use_Implications_for_Improving_Healthy_Eating_Practices/9986609 (accessed on 5 September 2021).
- Allison, D.B.; Basile, V.C.; Yuker, H.E. The measurement of attitudes toward and beliefs about obese persons. Int. J. Eat. Disord. 1991, 10, 599–607. [Google Scholar] [CrossRef]
- Ata, R.N.; Thompson, J.K.; Boepple, L.; Marek, R.J.; Heinberg, L.J. Obesity as a Disease: Effects on Weight-Biased Attitudes and Beliefs. Stigma Health 2018, 3, 406–416. [Google Scholar] [CrossRef] [Green Version]
- Mitchison, D.; Hay, P.; Griffiths, S.; Murray, S.B.; Bentley, C.; Gratwick-Sarll, K.; Harrison, C.; Mond, J. Disentangling body image: The relative associations of overvaluation, dissatisfaction, and preoccupation with psychological distress and eating disorder behaviors in male and female adolescents: Disentangling body image disturbance. Int. J. Eat. Disord. 2017, 50, 118–126. [Google Scholar] [CrossRef]
- Flynn, L.R.; Goldsmith, R.E. A Short, Reliable Measure of Subjective Knowledge. J. Bus. Res. 1999, 46, 57–66. [Google Scholar] [CrossRef]
- McGowan, L.; Pot, G.K.; Stephen, A.M.; Lavelle, F.; Spence, M.; Raats, M.; Hollywood, L.; McDowell, D.; McCloat, A.; Mooney, E.; et al. The influence of socio-demographic, psychological and knowledge-related variables alongside perceived cooking and food skills abilities in the prediction of diet quality in adults: A nationally representative cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutsuma, A.; Nakajima, K.; Suwa, K. Potential Association between Breakfast Skipping and Concomitant Late-Night-Dinner Eating with Metabolic Syndrome and Proteinuria in the Japanese Population. Scientifica 2014, 2014, 253581. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley: Boston, MA, USA, 1975. [Google Scholar]
- Naughton, P.; McCarthy, S.N.; McCarthy, M.B. The creation of a healthy eating motivation score and its association with food choice and physical activity in a cross sectional sample of Irish adults. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 74. [Google Scholar] [CrossRef] [Green Version]
- Brennan, L.; Binney, W.; Parker, L.; Aleti, T.; Nguyen, D. Social Marketing and Behaviour Change: Models, Theory and Applications; Edward Elgar: Cheltenham, UK; Northampton, MA, USA, 2014. [Google Scholar]
- Brennan, L.; Previte, J.; Fry, M.-L. Social marketing’s consumer myopia: Applying a behavioural ecological model to address wicked problems. J. Soc. Mark. 2016, 6, 219–239. [Google Scholar] [CrossRef]
- de Vet, E.; de Ridder, D.T.D.; de Wit, J.B.F. Environmental correlates of physical activity and dietary behaviours among young people: A systematic review of reviews. Obes. Rev. 2011, 12, e130–e142. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.E.; Sorensen, G.; Subramanian, S.V.; Kawachi, I. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grannell, A.; Fallon, F.; Al-Najim, W.; Roux, C. Obesity and responsibility: Is it time to rethink agency? Obes. Rev. 2021, 22, e13270. [Google Scholar] [CrossRef] [PubMed]
- Brennan, L.; Klassen, K.; Weng, E.; Chin, S.; Molenaar, A.; Reid, M.; Truby, H.; McCaffrey, T.A. A social marketing perspective of young adults’ concepts of eating for health: Is it a question of morality? Int. J. Behav. Nutr. Phys. Act. 2020, 17, 44. [Google Scholar] [CrossRef] [Green Version]
- Brennan, L.; Fry, M.-L.; Previte, J.; Chin, S. Consumers Have to Want to Change: Approach Versus Avoidance Strategies in Social Marketing to Counter Alcohol Consumption in Young People. In Proceedings of the 43rd Annual Macromarketing Conference: Change between Complexity and Simplicity, Leipzig, Germany, 9–12 July 2018. [Google Scholar]
- Hardcastle, S.J.; Hagger, M.S. Psychographic profiling for effective health behavior change interventions. Front. Psychol. 2016, 6, 1988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubacki, K.; Ronto, R.; Lahtinen, V.; Pang, B.; Rundle-Thiele, S. Social marketing interventions aiming to increase physical activity among adults: A systematic review. Health Educ. 2017, 117, 69–89. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.O.; Curry, L.E.; Fiacco, L.; Henes, A.; Farrelly, M.C.; Nonnemaker, J.M.; Hoffman, L.; Walker, M.W. Peer crowd segmentation for targeting public education campaigns: Hip hop youth and tobacco use. Prev. Med. Rep. 2019, 14, 100843. [Google Scholar] [CrossRef]
- Flynn, B.S.; Worden, J.K.; Bunn, J.Y.; Dorwaldt, A.L.; Connolly, S.W.; Ashikaga, T. Youth Audience Segmentation Strategies for Smoking-Prevention Mass Media Campaigns Based on Message Appeal. Health Educ. Behav. 2007, 34, 578–593. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Category | Lifestyle Mavens n = 311 (15.4%) | Health Conscious n = 425 (21.1%) | Aspirational Healthy Eaters n = 556 (27.5%) | Balanced All-Rounders n = 432 (21.4%) | Contemplating Another Day n = 226 (11.2%) | Blissfully Unconcerned n = 69 (3.4%) |
|---|---|---|---|---|---|---|---|
| Age (years) | 21 (2) | 21 (2) | 21 (2) | 21 (2) | 21 (2) | 21 (2) | |
| Ethnicity | Oceanian | 207 (66.6%) | 290 (68.2%) | 433 (77.9%) | 322 (74.5%) | 170 (75.2%) | 48 (69.6%) |
| Aboriginal or Torres Strait Islander | 11 (3.5%) | 15 (3.5%) | 17 (3.1%) | 13 (3.0%) | 11 (4.9%) | 6 (8.7%) | |
| North-West European | 19 (6.1%) | 27 (6.4%) | 42 (7.6%) | 42 (9.7%) | 9 (4.0%) | 2 (2.9%) | |
| Southern and Eastern European | 15 (4.8%) | 22 (5.2%) | 16 (2.9%) | 22 (5.1%) | 10 (4.4%) | 1 (1.4%) | |
| North African and Middle Eastern | 12 (3.9%) | 14 (3.3%) | 6 (1.1%) | 10 (2.3%) | 5 (2.2%) | 0 | |
| South-East Asian | 7 (2.3%) | 23 (5.4%) | 27 (4.9%) | 37 (8.6%) | 14 (6.2%) | 3 (4.3%) | |
| North-East Asian | 24 (7.7%) | 43 (10.1%) | 25 (4.5%) | 30 (6.9%) | 9 (4.0%) | 4 (5.8%) | |
| Southern and Central Asian | 28 (9%) | 21 (4.9%) | 35 (6.3%) | 23 (5.3%) | 15 (6.6%) | 3 (4.3%) | |
| Peoples of the Americas | 13 (4.2%) | 9 (2.1%) | 11 (2%) | 8 (1.9%) | 4 (1.8%) | 1 (1.4%) | |
| Sub-Saharan African | 8 (3.2%) | 6 (1.9%) | 1 (0.2%) | 4 (0.9%) | 3 (1.3%) | 0 | |
| Ethnicity Not Provided | 10 (3.2%) | 3 (0.7%) | 10 (1.8%) | 6 (1.4%) | 3 (1.3%) | 6 (8.7%) | |
| Education Level | Never attended school | 0 | 3 (0.7%) a | 1 (0.2%) a | 0 | 0 | 0 |
| Year 8 or below | 2 (0.6%) a | 2 (0.5%) a | 5 (0.9%) a | 3 (0.7%) a | 4 (1.8%) a | 1 (1.4%) a | |
| Year 9 or equivalent | 3 (1.0%) a,b | 1 (0.2%) a | 0 | 2 (0.5%) a | 1 (0.4%) a,b | 3b (4.3%) | |
| Year 10 or equivalent | 8 (2.6%) a,b | 12 (2.8%) a,b | 13 (2.3%) a | 19 (4.4%) a,b,c | 16 (7.1%) b,c | 9c (13.0%) | |
| Year 11 or equivalent | 10 (3.2%) a | 17 (4.0%) a | 26 (4.7%) a | 23 (5.3%) a | 15 (6.6%) a | 6 (8.7%) a | |
| Year 12 or equivalent | 92 (11.3%) a | 164 (38.6%) a,b | 255 (45.9%) b | 191 (44.2%) b,c | 93 (41.2%) a,b | 22 (31.9%) a,b | |
| Certificate (non-high school) | 6 (1.9%) a,b | 5 (1.2%) a,b | 7 (1.3%) a,b | 4 (0.9%) a | 2 (0.9%) a,b | 4 (5.8%) b | |
| Certificate I/II (non-high school) | 6 (1.9%) a,b | 8 (1.9%) a | 26 (4.7%) a,b | 17 (3.9%) a,b | 9 (4.0%) a,b | 6 (8.7%) b | |
| Certificate III/IV (non-high school) | 29 (9.3%) a | 40 (9.4%) a | 48 (8.6%) a | 49 (11.3%) a | 27 (11.9%) a | 1 (1.4%) a | |
| Advanced diploma/diploma | 19 (6.1%) a | 34 (8.0%) a | 41 (7.4%) a | 23 (5.3%) a | 23 (10.2%) a | 3 (4.3%) a | |
| Bachelor’s degree | 75 (18.4%) a | 109 (26.7%) a | 107 (19.2%) a,b | 78 (18.1%) a,b | 29 (12.8%) b | 10 (14.5%) a,b | |
| Graduate diploma/ graduate certificate | 18 (5.8%) a | 12 (2.8%) a | 13 (2.3%) a | 8 (1.9%) a | 5 (2.2%) a | 2 (2.9%) a | |
| Postgraduate degree | 37 (11.9%) a | 13 (3.1%) b | 11b (2.0%) b | 10 (2.3%) b | 2 (0.9%) b | 2 (2.9%) a,b | |
| Prefer not to say | 6 (1.9%) a | 5 (1.2%) a | 3 (0.5%) a | 5 (1.2%) a | 0 | 0 | |
| Weekly Income (AUD$) | No income | 24 (7.7%) a | 57 (13.4%) a,b | 59 (10.6%) a,c | 40 (18.1%) b,c | 40 (17.7%) b,c | 11 (15.9%) a,b |
| $1–$399 | 89 (28.6%) a | 114 (26.8%) a | 176 (31.7%) a | 71 (30.3%) a | 71 (31.4%) a | 30 (43.5%) a | |
| $400–$649 | 39 (12.5%) a | 66 (15.5%) a | 96 (17.3%) a | 28 (13.9%) a | 28 (12.4%) a | 7 (10.1%) a | |
| $650–$999 | 54 (17.4%) a | 59 (13.9%) a | 90 (16.2%) a | 34 (15.7%) a | 34 (15.0%) a | 6 (8.7%) a | |
| $1000–$1499 | 46 (14.8%) a | 63 (14.8%) a | 46 (8.3%) b | 23 (10.0%) a,b | 23 (10.2%) a,b | 7 (10.1%) a,b | |
| $1500–over $3000 | 47 (15.1%) a | 45 (10.6%) a,b | 47 (8.5%) b,c | 14 (4.4%) b,c,d | 14 (6.2%) b,c,d | 3 (4.3%) a,b,c | |
| Prefer not to say | 12 (9.3%) a | 21 (4.9%) a | 42 (7.6%) a | 16 (7.6%) a | 16 (7.1%) a | 5 (7.2%) a | |
| Living Arrangements | One family household with only family members present | 142 (45.7%) | 192 (21.2%) | 252 (45.3%) | 192 (44.4%) | 97 (42.9%) | 29 (42.0%) |
| Two family household with only family members present | 16 (5.1%) | 24 (5.6%) | 30 (5.4%) | 23 (5.3%) | 11 (4.9%) | 2 (2.9%) | |
| Three or more family household with only family members present | 21 (6.6%) | 54 (12.7%) | 65 (11.7%) | 51 (11.8%) | 28 (12.4%) | 4 (5.8%) | |
| One family household with non-family members present | 6 (1.9%) | 18 (4.2%) | 20 (3.6%) | 20 (4.8%) | 8 (3.5%) | 1 (1.4%) | |
| Two family household with non-family members present | 9 (2.9%) | 5 (1.2%) | 19 (3.4%) | 10 (2.3%) | 7 (3.1%) | 0 | |
| Three or more family household with non-family members present | 18 (5.8%) | 17 (4.0%) | 21 (3.8%) | 14 (3.2%) | 6 (2.7%) | 3 (4.3%) | |
| Lone person household | 38 (12.2%) | 44 (10.4%) | 39 (7.0%) | 40 (9.3%) | 25 (11.1%) | 13 (18.8%) | |
| Group household | 36 (11.6%) | 50 (11.8%) | 75 (13.5%) | 62 (14.4%) | 31 (13.7%) | 10 (14.5%) | |
| Prefer not to say | 25 (8.0%) | 21 (4.9%) | 35 (6.3%) | 20 (4.6%) | 13 (5.8%) | 7 (10.0%) | |
| Studying Status | Studying full-time | 111 (35.7%) | 151 (35.5%) | 191 (34.4%) | 170 (39.4%) | 95 (42%) | 13 (18.8%) |
| Studying part-time | 60 (19.3%) | 86 (20.2%) | 106 (19.1%) | 68 (15.7%) | 36 (15.9%) | 13 (18.8%) | |
| Not studying | 122 (39.2%) | 173 (21.1%) | 233 (41.9%) | 174 (40.3%) | 82 (36.3%) | 36 (52.2%) | |
| Prefer not to say | 11 (3.5%) | 8 (1.9%) | 11 (2.0%) | 9 (2.1%) | 8 (3.5%) | 6 (8.7%) | |
| Working Status | Working full-time | 144 (46.3%) | 141 (33.2%) | 140 (25.2%) | 95 (22.0%) | 39 (17.3%) | 13 (18.8%) |
| Working part-time | 75 (24.1%) | 111 (26.1%) | 155 (27.9%) | 97 (22.5%) | 53 (23.5%) | 13 (18.8%) | |
| Working casually | 33 (10.6%) | 64 (15.1%) | 102 (18.3%) | 92 (21.3%) | 39 (17.3%) | 12 (17.4%) | |
| Not working | 50 (16.1%) | 101 (23.8%) | 146 (26.3%) | 138 (31.9%) | 90 (39.8%) | 26 (37.7%) | |
| Prefer not to say | 8 (2.6%) | 5 (1.2%) | 12 (2.2%) | 8 (1.9%) | 4 (1.8%) | 5 (7.2%) | |
| Body Mass Index (kg/m2) | 24.58 a,d,e (5.93) | 23.40 (4.86) a | 26.04 (6.66) c | 23.73 (4.94) a,b | 25.39 (6.32) c,d | 26.27 (7.34) b,c,e | |
| BMI Categories | Underweight (BMI < 18.5) | 28 (9.0%) | 42 (9.9%) | 37 (6.7%) | 41 (9.5%) | 16 (7.1%) | 9 (13.0%) |
| Healthy weight (BMI 18.5–24.9) | 171 (55.0%) | 275 (64.7%) | 260 (46.8%) | 254 (58.8%) | 111 (49.1%) | 30 (43.5%) | |
| Overweight (BMI 25.0–29.9) | 72 (23.2%) | 76 (17.9%) | 145 (26.1%) | 87 (20.1%) | 53 (23.5%) | 13 (18.8%) | |
| Obese (BMI >30.0) | 40 (12.9%) | 32 (7.5%) | 114 (20.5%) | 50 (11.6%) | 46 (20.4%) | 17 (24.6%) |
| Characteristic | Maximum Score | Lifestyle Mavens n = 311 (15.4%) | Health Conscious n = 425 (21.1%) | Aspirational Healthy Eaters n = 556 (27.5%) | Balanced All-Rounders n = 432 (21.4%) | Contemplating Another Day n = 226 (11.2%) | Blissfully Unconcerned n = 69 (3.4%) |
|---|---|---|---|---|---|---|---|
| Cause of obesity—Energy imbalance | 10 | 7.0 (2.06) a,c | 7.3 (1.87) a,b | 7.2 (1.84) a,b,d | 7.5 (1.86) b | 7.2 (1.87) a,b,d | 6.4 (2.12) c,d |
| Cause of obesity—Medical | 10 | 7.4 (1.84) a,b | 7.8 (3.06) a,c | 7.9 (1.49) c,d | 8.2 (1.51) d | 7.9 (1.59) c,d | 6.9 (2.09) b |
| Cause of obesity—Willpower | 5 | 2.8 (1.18) a | 3.1 (1.12) a,b | 3.3 (3.25) b,d | 3.3 (1.06) b,c,d | 3.4 (1.05) d | 3.2 (1.16) a,b,d |
| Characteristic | Maximum Score | Lifestyle Mavens n = 311 (15.4%) | Health Conscious n = 425 (21.1%) | Aspirational Healthy Eaters n = 556 (27.5%) | Balanced All-Rounders n = 432 (21.4%) | Contemplating Another Day n = 226 (11.2%) | Blissfully Unconcerned n = 69 (3.4%) |
|---|---|---|---|---|---|---|---|
| Self-perception of cooking | 35 | 23.5 (5.1) a | 23.6 (5.73) a | 22.3 (5.98) b,d | 22.7 (6.17) a,b | 20.4 (6.30) c | 19.9 (6.37) c,d |
| Choosing healthy foods | 5 | 4 (1) a | 4 (1) a | 3 (1) b | 3 (1) b | 2 (1) c | 2 (1) c |
| Meal planning and prepping food | 15 | 10.4 (2.48) a,c | 10.6 (2.25) a | 9.7 (2.41) b,e | 10.0 (2.64) b,c | 8.7 (2.12) d | 8.8 (2.53) d,e |
| Shopping | 15 | 10.4 (2.55) a | 10.7 (2.66) a | 9.8 (2.81) b | 10.4 (3.06) a | 9.5 (2.82) b | 9.0 (2.53) c |
| Budgeting | 20 | 14.0 (3.12) a | 14.1 (3.13) a | 13.0 (3.64) b | 13.8 (3.86) a | 12.4 (3.86) b,c | 11.2 (3.59) c |
| Label comprehension and use | 20 | 14.2 (3.08) a | 14.9 (3.19) a | 13.5 (3.17) b | 14.2 (3.39) a | 12.5 (3.30) c | 11.38 (2.93) c |
| Resourcefulness | 25 | 17.7 (3.67) a | 18.1 (3.81) a | 16.6 (4.09) b | 17.7 (4.02) a | 15.6 (4.30) b,c | 14.3 (4.0) c |
| Characteristic | Maximum Score | Lifestyle Mavens n = 311 (15.4%) | Health Conscious n = 425 (21.1%) | Aspirational Healthy Eaters n = 556 (27.5%) | Balanced All-Rounders n = 432 (21.4%) | Contemplating Another Day n = 226 (11.2%) | Blissfully Unconcerned n = 69 (3.4%) |
|---|---|---|---|---|---|---|---|
| Subjective norms to healthy eating | 15 | 8.4 (3.19) a,d | 7.6 (3.04) b | 9.1 (2.81) c | 7.8 (3.02) a,b | 9.2 (2.70) c | 9.5 (3.07) c,d |
| Motivation to comply | 15 | 10.3 (2.61) a | 10.3 (2.51) a | 9.7 (2.42) b | 9.7 (2.73) b | 8.9 (2.47) d | 8.3 (2.54) d |
| Current satisfaction with healthy eating | 15 | 10.2 (2.58) a | 10.2 (2.37) a | 7.5 (2.38) b | 9.1 (2.66) c | 7.4 (2.52) b | 7.7 (2.34) b |
| Positive attitudes towards healthy eating | 10 | 7.3 (2.14) a | 8.1 (1.82) b,c | 7.9 (1.60) b | 8.3 (1.57) c | 7.5 (1.61) a | 6.5 (1.91) d |
| Heathy eating is difficult | 5 | 3.0 (1.22) a,d | 3.3 (1.14) b | 2.6 (1.01) c | 3.1 (1.15) a,b | 2.6 (1.09) c | 2.6 (1.09) c,d |
| Self-efficacy | 15 | 11.3 (2.64) a,c | 11.7 (2.40) a,b | 11.4 (2.35) a | 12.1 (2.40) b | 11.4 (2.44) a | 10.3 (2.57) c |
| Perceived nutrition knowledge/expertise | 20 | 13.5 (3.52) a | 14.5 (3.18) b | 13.5 (3.32) a | 14.5 (3.24) b | 13.1 (3.52) a,c | |
| Nutrition knowledge Mavenism | 10 | 6.9 (1.71) a | 6.2 (1.76) b | 5.0 (2.02) c | 5.0 (2.07) c | 4.1 (1.92) d | 4.4 (1.89) c,d |
| Intention towards healthy eating | 15 | 10.5 (2.6) a | 10.6 (2.89) a | 11.1 (2.59) b | 10.1 (3.14) a | 9.1(3.02) c | 7.7(3.05) d |
| Unhealthy eating habits (skipping breakfast during week) | 5 | 2.8 (1.28) a | 2.9 (1.43) a | 3.2 (1.49) b,c | 3.0 (1.63) a,b | 3.4 (1.48) c | 3.5 (1.30) b,c |
| Unhealthy eating habits (dinner before bed during week) | 5 | 3.0 (1.2) a | 2.9 (1.23) a | 2.9 (1.35) a | 2.8 (1.45) a | 3.0 (1.38) a | 3.2 (1.19) a |
| Unhealthy eating habits (skipping breakfast during weekend) | 5 | 2.9 (1.25) a,b | 2.8 (1.42) a | 3.2 (1.50) b,d | 2.9 (1.64) a,b | 3.3 (1.50) b,c,d | 3.6 (1.25) d |
| Unhealthy eating habits (dinner before bed during weekend) | 5 | 3.2 (1.20) a | 2.8 (1.27) b,c | 2.9 (1.40) b | 2.6 (1.46) c | 2.8 (1.39) b,c | 3.1 (1.17) a,b,c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dix, C.F.; Brennan, L.; Reid, M.; McCaffrey, T.A.; Molenaar, A.; Barklamb, A.; Chin, S.; Truby, H. Nutrition Meets Social Marketing: Targeting Health Promotion Campaigns to Young Adults Using the Living and Eating for Health Segments. Nutrients 2021, 13, 3151. https://doi.org/10.3390/nu13093151
Dix CF, Brennan L, Reid M, McCaffrey TA, Molenaar A, Barklamb A, Chin S, Truby H. Nutrition Meets Social Marketing: Targeting Health Promotion Campaigns to Young Adults Using the Living and Eating for Health Segments. Nutrients. 2021; 13(9):3151. https://doi.org/10.3390/nu13093151
Chicago/Turabian StyleDix, Clare F., Linda Brennan, Mike Reid, Tracy A. McCaffrey, Annika Molenaar, Amy Barklamb, Shinyi Chin, and Helen Truby. 2021. "Nutrition Meets Social Marketing: Targeting Health Promotion Campaigns to Young Adults Using the Living and Eating for Health Segments" Nutrients 13, no. 9: 3151. https://doi.org/10.3390/nu13093151