Your new post is loading...
Your new post is loading...

|
Scooped by
nrip
|
COVID-19 Research Resources to develop your own study materials
The Covid-19 Research Implementation and Knowledge Hub of the Global Health Network contains a wide range of resources to guide teams in developing their own study materials and support high-quality, rapid implementation of critical COVID-19 studies in various settings. The Global Health Network is running this crowdsourcing initiative to support a faster implementation of research studies during this pandemic. It slow and unnecessary for each group wanting to set up a study to start from scratch; when there are excellent studies already running. The Hub is being continually updated so its good to bookmark it so you can check it regularly for new resources that could help your research team with your COVID-19 study. Link to the Covid-19 Research Implementation and Knowledge Hub
|
|
Scooped by
nrip
|
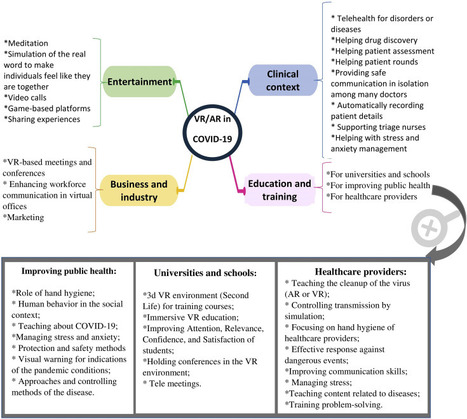
The pandemics of major infectious diseases often cause public health, economic, and social problems. Virtual reality (VR) and augmented reality (AR), as two novel technologies, have been used in many fields for emergency management of disasters. The objective of this paper was to review VR and AR applications in the emergency management of infectious outbreaks with an emphasis on the COVID-19 outbreak. It appears that VR and AR technologies can play a positive role during infectious disease outbreaks. VR and AR have been widely used in the prevention and response phases of emergency management during infectious disease pandemics, such as SARS and Ebola pandemics, especially for educating and training purposes for the public. During the COVID-19 outbreak, these technologies have the potential to be used in various fields, including 1) clinical context (e.g., telehealth, drug discovery, patient assessment, mental health management), 2) entertainment (e.g., video call, meditation, gaming), 3) business and industry (e.g., holding meetings and conferences, marketing), and 4) education (e.g., in schools and universities, for healthcare providers, and VR-based content for improving public health). These technologies can be used in the above-mentioned fields by providing their different features for facilitating the challenges of COVID-19. However, to respond to COVID-19, all applications of VR and AR should be considered as a supportive approach alongside other information technologies. We believe that VR and AR have a substantial potential to impact the emergency management of COVID-19 or any infectious disease pandemics; however, these potentials need to be studied in a more robust manner. read the paper ta https://www.sciencedirect.com/science/article/pii/S2352914821000691
|
|
Scooped by
nrip
|
The national severe acute respiratory illness (SARI) surveillance system in Yemen was established in 2010 to monitor SARI occurrence in humans and provide a foundation for detecting SARI outbreaks. This study aimed to examine the level of usefulness and the performance of the SARI surveillance system in Yemen.
Methods: The updated Centers for Disease Control and Prevention guidelines were used for the purposes of our evaluation. Related documents and reports were reviewed. Data were collected from 4 central-level managers and stakeholders and from 10 focal points at 4 sentinel sites by using a semistructured questionnaire.
For each attribute, percent scores were calculated and ranked as follows: very poor (≤20%), poor (20%-40%), average (40%-60%), good (60%-80%), and excellent (>80%). The surveillance systems at sentinel sites are tools for the early detection of disease, the monitoring of trends in the burden of diseases, and the generation of recommendations for the prevention and control of diseases. The evaluation of surveillance systems helps decision makers to set priorities for future planning, resource allocation, and future interventions for preventing the spread of diseases.
Results: As rated by the evaluators, the SARI surveillance system achieved its objectives.
The system’s flexibility (percent score: 86%) and acceptability (percent score: 82%) were rated as “excellent,” and simplicity (percent score: 74%) and stability (percent score: 75%) were rated as “good.” The percent score for timeliness was 23% in 2018, which indicated poor timeliness. The overall data quality percent score of the SARI system was 98.5%. Despite its many strengths, the SARI system has some weaknesses. For example, it depends on irregular external financial support.
The SARI surveillance system was useful in estimating morbidity and mortality, monitoring the trends of the disease, and promoting research for informing prevention and control measures.
The overall performance of the SARI surveillance system was good. We recommend expanding the system by promoting private health facilities’ (eg, private hospitals and private health centers) engagement in SARI surveillance, establishing an electronic database at central and peripheral sites, and providing the National Central Public Health Laboratory with the reagents needed for disease confirmation.
|
|
Scooped by
nrip
|
Agencies such as the Centers for Disease Control and Prevention (CDC) currently release influenza-like illness incidence data, along with descriptive summaries of simple spatio-temporal patterns and trends. However, public health researchers, government agencies, as well as the general public, are often interested in deeper patterns and insights into how the disease is spreading, with additional context. Analysis by domain experts is needed for deriving such insights from incidence data.
Objective: Our goal was to develop an automated approach for finding interesting spatio-temporal patterns in the spread of a disease over a large region, such as regions which have specific characteristics (eg, high incidence in a particular week, those which showed a sudden change in incidence) or regions which have significantly different incidence compared to earlier seasons.
Methods: We developed techniques from the area of transactional data mining for characterizing and finding interesting spatio-temporal patterns in disease spread in an automated manner. A key part of our approach involved using the principle of minimum description length for representing a given target set in terms of combinations of attributes (referred to as clauses); we considered both positive and negative clauses, relaxed descriptions which approximately represent the set, and used integer programming to find such descriptions. Finally, we designed an automated approach, which examines a large space of sets corresponding to different spatio-temporal patterns, and ranks them based on the ratio of their size to their description length (referred to as the compression ratio).
Results: We applied our methods using minimum description length to find spatio-temporal patterns in the spread of seasonal influenza in the United States using state level influenza-like illness activity indicator data from the CDC. We observed that the compression ratios were over 2.5 for 50% of the chosen sets, when approximate descriptions and negative clauses were allowed. Sets with high compression ratios (eg, over 2.5) corresponded to interesting patterns in the spatio-temporal dynamics of influenza-like illness. Our approach also outperformed description by solution in terms of the compression ratio.
Conclusions: Our approach, which is an unsupervised machine learning method, can provide new insights into patterns and trends in the disease spread in an automated manner. Our results show that the description complexity is an effective approach for characterizing sets of interest, which can be easily extended to other diseases and regions beyond influenza in the US. Our approach can also be easily adapted for automated generation of narratives. read more at https://publichealth.jmir.org/2020/3/e12842
We discuss the concept of a participatory digital contact notification approach to assist tracing of contacts who are exposed to confirmed cases of coronavirus disease (COVID-19); The core functionality of our concept is to provide a usable, labor-saving tool for contact tracing by confirmed cases themselves the approach is simple and affordable for countries with limited access to health care resources and advanced technology. The proposed tool serves as a supplemental contract tracing approach to counteract the shortage of health care staff while providing privacy protection for both cases and contacts. - This tool can be deployed on the internet or as a plugin for a smartphone app.
- Confirmed cases with COVID-19 can use this tool to provide contact information (either email addresses or mobile phone numbers) of close contacts.
- The system will then automatically send a message to the contacts informing them of their contact status, what this status means, the actions that should follow (eg, self-quarantine, respiratory hygiene/cough etiquette), and advice for receiving early care if they develop symptoms.
- The name of the sender of the notification message by email or mobile phone can be anonymous or not.
- The message received by the contact contains no disease information but contains a security code for the contact to log on the platform to retrieve the information.
Conclusion The successful application of this tool relies heavily on public social responsibility and credibility, and it remains to be seen if the public would adopt such a tool and what mechanisms are required to prevent misuse. This is a simple tool that does not require complicated computer techniques despite strict user privacy protection design with respect to countries and regions. Additionally, this tool can help avoid coercive surveillance, facilitate the allocation of health resources, and prioritize clinical service for patients with COVID-19. Information obtained from the platform can also increase our understanding of the epidemiology of COVID-19. read this concept paper at https://mhealth.jmir.org/2020/6/e20369
|
|
Scooped by
nrip
|
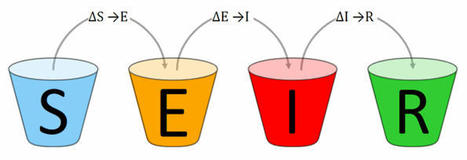
Pandemic SEIR and SEIRV modelling software and infrastructure for the Corona SARS-COV-2 COVID-19 disease with data from Johns-Hopkins-University CSSE, Robert Koch-Institute and vaccination data from Our World In Data. The SARS-COV-2 pandemic has been affecting our lives for months. The effectiveness of measures against the pandemic can be tested and predicted by using epidemiological models. The Corona SEIR Workbench uses a SEIR model and combines a graphical output of the results with a simple parameter input for the model. Modelled data can be compared country by country with the SARS-COV-2 infection data of the Johns Hopkins University. Additionally, the R₀ values of the Robert Koch Institute can be displayed for Germany. Vaccination data is used from Our World In Data.
|
|
Scooped by
nrip
|
Despite recent achievements in vaccines, antiviral drugs, and medical infrastructure, the emergence of COVID-19 has posed a serious threat to humans worldwide. Most countries are well connected on a global scale, making it nearly impossible to implement perfect and prompt mitigation strategies for infectious disease outbreaks. In particular, due to the explosive growth of international travel, the complex network of human mobility enabled the rapid spread of COVID-19 globally.
Objective:
South Korea was one of the earliest countries to be affected by COVID-19. In the absence of vaccines and treatments, South Korea has implemented and maintained stringent interventions, such as large-scale epidemiological investigations, rapid diagnosis, social distancing, and prompt clinical classification of severely ill patients with appropriate medical measures. In particular, South Korea has implemented effective airport screenings and quarantine measures. In this study, we aimed to assess the country-specific importation risk of COVID-19 and investigate its impact on the local transmission of COVID-19. Methods: The country-specific importation risk of COVID-19 in South Korea was assessed. We investigated the relationships between country-specific imported cases, passenger numbers, and the severity of country-specific COVID-19 prevalence from January to October 2020. We assessed the country-specific risk by incorporating country-specific information. A renewal mathematical model was employed, considering both imported and local cases of COVID-19 in South Korea. Furthermore, we estimated the basic and effective reproduction numbers.
Results: The risk of importation from China was highest between January and February 2020, while that from North America (the United States and Canada) was high from April to October 2020. The R0 was estimated at 1.87 (95% CI 1.47-2.34), using the rate of α=0.07 for secondary transmission caused by imported cases. The Rt was estimated in South Korea and in both Seoul and Gyeonggi.
Conclusions: A statistical model accounting for imported and locally transmitted cases was employed to estimate R0 and Rt.
Our results indicated that the prompt implementation of airport screening measures (contact tracing with case isolation and quarantine) successfully reduced local transmission caused by imported cases despite passengers arriving from high-risk countries throughout the year. Moreover, various mitigation interventions, including social distancing and travel restrictions within South Korea, have been effectively implemented to reduce the spread of local cases in South Korea. read the paper at https://publichealth.jmir.org/2021/6/e26784/
|
|
Scooped by
nrip
|
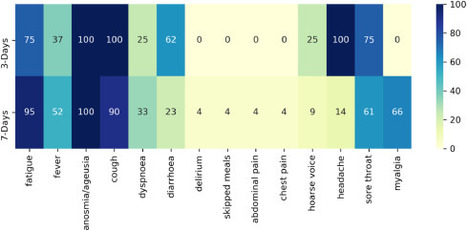
In a clinical trial, diagnostic testing of suspected cases e.g RT-PCR for severe acute respiratory SARS-CoV-2, can be triggered by the presence of any COVID-19 associated symptom.
A household survey in the United Kingdom (UK) showed that fever, cough, anosmia, and ageusia were present on the day of testing in only 60% of symptomatic, RT-PCR positive individuals, implying that other less specific signs/symptoms associated with COVID-19 occur in a substantial number of patients.
The signs/symptoms associated with COVID-19 are extensive and overlap with those of other common viral infections.
Diagnostic work-up following any COVID-19 associated symptom will lead to extensive testing, potentially overwhelming laboratory capacity whilst primarily yielding negative results. We aimed to identify optimal symptom combinations to capture most cases using fewer tests with implications for COVID-19 vaccine developers across different resource settings and public health.
Methods
UK and US users of the COVID-19 Symptom Study app who reported new-onset symptoms and an RT-PCR test within seven days of symptom onset were included. Sensitivity, specificity, and number of RT-PCR tests needed to identify one case (test per case [TPC]) were calculated for different symptom combinations.
A multi-objective evolutionary algorithm was applied to generate combinations with optimal trade-offs between sensitivity and specificity.
Interpretation
We confirmed the significance of COVID-19 specific symptoms for triggering RT-PCR and identified additional symptom combinations with optimal trade-offs between sensitivity and specificity that maximize case capture given different resource settings.
read this paper at https://www.journalofinfection.com/article/S0163-4453(21)00079-7/fulltext
|
|
Scooped by
nrip
|
Given the potential for the evolution of SARS-CoV-2 variants that render vaccines less effective (vaccine escape), assisted by waning immunity following vaccination, how can COVID-19 exit strategies be planned while limiting the vaccine escape risk? A key component of any plausible strategy towards the permanent removal of non-pharmaceutical interventions (NPIs) is ensuring low case numbers in the short to medium term using NPIs and vaccination. Read this paper which discusses this mathematically https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00202-4/fulltext
|
|
Scooped by
nrip
|
The COVID-19 pandemic consistently demonstrated a pattern of growing community transmission worldwide, even with the adoption of social distancing measures (lockdown or voluntarily shelter in place) in January and early May 2020. The continuing transmission of the virus despite the policy measures adopted in some countries was an important point of debate and investigation in the scientific community and among authorities. Unexpected forms of transmission (atmospheric) associated with the social distancing policy became the central question for the infectious transmission modeling of SARS-CoV-2 and predictive methods. Daily new COVID-19 cases from January to April 2020 demonstrate varying patterns of SARS-CoV-2 transmission across different geographical regions. China and South Korea successfully and quickly flattened their COVID-19 curve. To understand why this was the case, this paper investigated possible aerosol-forming patterns in the atmosphere and their relationship to the policy measures adopted by select countries.
Objective: The main research objective was to compare the outcomes of policies adopted by countries between January and April 2020. Policies included physical distancing measures that in some cases were associated with mask use and city disinfection. We investigated whether the type of social distancing framework adopted by some countries (ie, without mask use and city disinfection) led to the continual dissemination of SARS-CoV-2 (daily new cases) in the community during the study period.
Methods: We examined the policies used as a preventive framework for virus community transmission in some countries and compared them to the policies adopted by China and South Korea. Countries that used a policy of social distancing by 1-2 m were divided into two groups. The first group consisted of countries that implemented social distancing (1-2 m) only, and the second comprised China and South Korea, which implemented distancing with additional transmission/isolation measures using masks and city disinfection. Global daily case maps from Johns Hopkins University were used to provide time-series data for the analysis.
Results: The results showed that virus transmission was reduced due to policies affecting SARS-CoV-2 propagation over time. Remarkably, China and South Korea obtained substantially better results than other countries at the beginning of the epidemic due to their adoption of social distancing (1-2 m) with the additional use of masks and sanitization (city disinfection). These measures proved to be effective due to the atmosphere carrier potential of SARS-CoV-2 transmission.
Conclusions: Our findings confirm that social distancing by 1-2 m with mask use and city disinfection yields positive outcomes. These strategies should be incorporated into prevention and control policies and be adopted both globally and by individuals as a method to fight the COVID-19 pandemic.
read the study at https://publichealth.jmir.org/2021/4/e20699/
|
|
Scooped by
nrip
|
The Centers for Disease Control and Prevention (CDC) warned in a document published Friday of "repeatedly documented" instances of coronavirus spreading through the air to people more than 6 feet away under certain conditions. The new document explaining the latest understanding of how the virus spreads is part of a shifting emphasis towards airborne transmission of the virus. "Transmission of SARS-CoV-2 from inhalation of virus in the air farther than six feet from an infectious source can occur," the new document says in large letters, while noting it is "less likely than at closer distances." Some experts have been pushing the CDC for months to place a greater emphasis on airborne transmission and the need to improve ventilation, even with something as simple as opening the window in a room. Experts have also long said that outdoors is far safer than indoors. The CDC acknowledged last year that the virus can spread through airborne transmission, but there has since been a growing emphasis on that method of transmission. The agency emphasized that while it is updating its understanding of how the virus spreads, the same methods for keeping safe still apply. Wearing a mask, distancing from others, avoiding crowded indoor areas and allowing adequate ventilation are recommended. read the story at https://thehill.com/policy/healthcare/552406-cdc-warns-virus-can-spread-more-than-six-feet-under-certain-conditions
|
|
Scooped by
nrip
|
The spread of SARS-CoV-2, originating in Wuhan, China, was classified as a pandemic by the World Health Organization on March 11, 2020. The governments of affected countries have implemented various measures to limit the spread of the virus. The starting point of this paper is the different government approaches, in terms of promulgating new legislative regulations to limit the virus diffusion and to contain negative effects on the populations. Objective: This paper aims to study how the spread of SARS-CoV-2 is linked to government policies and to analyze how different policies have produced different results on public health.
Methods: Considering the official data provided by 4 countries (Italy, Germany, Sweden, and Brazil) and from the measures implemented by each government, we built an agent-based model to study the effects that these measures will have over time on different variables such as the total number of COVID-19 cases, intensive care unit (ICU) bed occupancy rates, and recovery and case-fatality rates. The model we implemented provides the possibility of modifying some starting variables, and it was thus possible to study the effects that some policies (eg, keeping the national borders closed or increasing the ICU beds) would have had on the spread of the infection.
Conclusions: In line with what we expected, the obtained results showed that the countries that have taken restrictive measures in terms of limiting the population mobility have managed more successfully than others to contain the spread of COVID-19. Moreover, the model demonstrated that herd immunity cannot be reached even in countries that have relied on a strategy without strict containment measures.
read the study at https://medinform.jmir.org/2021/4/e24192
|
|
Scooped by
nrip
|
Sentinel surveillance of influenza-like illness (ILI) in Egypt started in 2000 at 8 sentinel sites geographically distributed all over the country. In response to the COVID-19 pandemic, SARS-CoV-2 was added to the panel of viral testing by polymerase chain reaction (PCR) for the first 2 patients with ILI seen at one of the sentinel sites. We report the first SARS-CoV-2 and influenza A(H1N1) virus co-infection with mild symptoms detected through routine ILI surveillance in Egypt.
This report aims to describe how the case was identified and the demographic and clinical characteristics and outcomes of the patient.
Conclusions: This case highlights the possible occurrence of SARS-CoV-2/influenza A(H1N1) co-infection in younger and healthy people, who may resolve the infection rapidly. We emphasize the usefulness of the surveillance system for detection of viral causative agents of ILI and recommend broadening of the testing panel, especially if it can guide case management.
read the paper at https://publichealth.jmir.org/2021/4/e27433
|
Digital tools are increasingly being applied to support the response to the ongoing COVID-19 pandemic in India and elsewhere globally. This article draws from global frameworks to explore the use of digital tools in the state of Kerala across the domains of communication, surveillance, clinical management, non-clinical support, and core health system readiness and response. Kerala is considered India’s first digital state, with the highest percentage of households with computers (24%) and the internet (51%) in India, 95% mobile phone penetration, 62% smartphone penetration and 75% digital literacy. Kerala has long been a model for the early adoption of digital technology for education and health. As part of the pandemic response, technology has been used across private and public sectors, including law enforcement, health, information technology and education. Efforts have sought to ensure timely access to health information, facilitate access to entitlements, monitor those under quarantine and track contacts, and provide healthcare services though telemedicine. Kerala’s COVID-19 pandemic response showcases the diverse potential of digital technology, the importance of building on a strong health system foundation, the value of collaboration, and the ongoing challenges of data privacy and equity in digital access. Summary -
The COVID-19 pandemic’s unprecedented global spread and impact has accelerated interest in digital innovation. -
Kerala’s experience showcases the diverse and innovative ways that digital tools can build on a strong underlying health system to support pandemic response across the domains of communication, surveillance, clinical management, non-clinical support and core health system readiness. -
Digital tools in Kerala were able to proliferate rapidly and help meet diverse citizen needs due to high levels of collaboration and intersectoral response that brought together different levels of government and multiple state departments, engaged the private sector, and harnessed the energy of civil society organisations and community volunteers. -
Digital technology has great potential to strengthen public health measures during pandemics, including to rapidly link citizens to food and mental health support. -
Adequate oversight and community participation remains essential to safeguard citizen privacy and ensure equity. read the open access paper at https://gh.bmj.com/content/6/Suppl_5/e005355
|
|
Scooped by
nrip
|
A team of researchers analyzed the genomes of more than 2,500 modern humans from 26 worldwide populations, to better understand how humans have adapted to historical coronavirus outbreaks. The team used computational methods to uncover genetic traces of adaptation to coronaviruses, the family of viruses responsible for three major outbreaks in the last 20 years, including the ongoing COVID-19 pandemic. Traces of the outbreak are evident in the genetic makeup of people from that area, they’ve found. A coronavirus epidemic broke out in the East Asia region more than 20,000 years ago, as per their findings. The discovery of a coronavirus outbreak from 20,000 years ago is "like finding fossilized dinosaur footprints instead of finding fossilized bones directly. The work shows that over the course of the epidemic, selection favored certain variants of human genes involved in the virus-cell interactions that could have led to a less severe disease. Studying the “tracks” left by ancient viruses can help researchers better understand how the genomes of different human populations adapted to viruses that have emerged as important drivers of human evolution. The study’s authors say their research could help identify viruses that have caused epidemics in the distant past and may do so in the future. Studies like theirs help researchers compile a list of potentially dangerous viruses and then develop diagnostics, vaccines, and drugs for the event of their return. read the paper at https://www.cell.com/current-biology/fulltext/S0960-9822(21)00794-6 more at https://www.futurity.org/coronavirus-epidemic-viruses-2597742/
|
|
Scooped by
nrip
|
This study aims to describe the compounding factors in a complex emergency, which exacerbate a cholera epidemic among vulnerable populations due to supply chain disruptions. Basic needs such as food, medicine, water, sanitation and hygiene commodities are critical to reduce the incidence rate of cholera and control the spread of infection. Conflicts cause damage to infrastructure, displace vulnerable populations and restrict the flow of goods from both commercial and humanitarian organizations. This study assesses the underlying internal and external factors that either aggravate or mitigate the risk of a cholera outbreak in such settings, using Yemen as a case study. Findings Compounding factors that influenced the cholera outbreak in Yemen are visualized in a causal loop diagram, which can improve the understanding of relationships where numerous uncertainties exist. A strong link exists between humanitarian response and the level of infrastructure development in a country. Supply chains are affected by constraints deriving from the Yemeni conflict, further inhibiting the use of infrastructure, which limits access to basic goods and services. Aligning long-term development objectives with short-term humanitarian response efforts can create more flexible modes of assistance to prevent and control future outbreaks. Practical implications This study presents a systematic view of dynamic factors existing in complex emergencies that have cause-and-effect relationships. Several models of cholera outbreaks have been used in previous studies, primarily focusing on the modes and mechanisms of transmission throughout a population. However, such models typically do not include other internal and external factors that influence the population and context at the site of an outbreak. This model incorporates those factors from a logistics perspective to address the distribution of in-kind goods and cash and voucher assistance. Social implications This study has been aligned with six of the United Nations Sustainable Development Goals (SDGs), using their associated targets in the model as variables that influence the cholera incidence rate. Recognizing that the SDGs are interlinked, as are the dynamic factors in complex humanitarian emergencies, the authors have chosen to take an interdisciplinary approach to consider social, economic and environmental factors that may be impacted by this research. read more at https://www.emerald.com/insight/content/doi/10.1108/JHLSCM-07-2020-0063/full/html
The COVID-19 pandemic is the greatest public health crisis of the last 100 years. Countries have responded with various levels of lockdown to save lives and stop health systems from being overwhelmed. At the same time, lockdowns entail large socioeconomic costs. One exit strategy under consideration is a mobile phone app that traces the close contacts of those infected with COVID-19. Recent research has demonstrated the theoretical effectiveness of this solution in different disease settings. However, concerns have been raised about such apps because of the potential privacy implications. This could limit the acceptability of app-based contact tracing in the general population. As the effectiveness of this approach increases strongly with app uptake, it is crucial to understand public support for this intervention. Objective: The objective of this study is to investigate the user acceptability of a contact-tracing app in five countries hit by the pandemic.
Methods: We conducted a largescale, multicountry study (N=5995) to measure public support for the digital contact tracing of COVID-19 infections.
We ran anonymous online surveys in France, Germany, Italy, the United Kingdom, and the United States and measured intentions to use a contact-tracing app across different installation regimes (voluntary installation vs automatic installation by mobile phone providers) and studied how these intentions vary across individuals and countries.
Results: We found strong support for the app under both regimes, in all countries, across all subgroups of the population, and irrespective of regional-level COVID-19 mortality rates.
We investigated the main factors that may hinder or facilitate uptake and found that concerns about cybersecurity and privacy, together with a lack of trust in the government, are the main barriers to adoption.
Conclusions:
Epidemiological evidence shows that app-based contact tracing can suppress the spread of COVID-19 if a high enough proportion of the population uses the app and that it can still reduce the number of infections if uptake is moderate. Our findings show that the willingness to install the app is very high. The available evidence suggests that app-based contact tracing may be a viable approach to control the diffusion of COVID-19. read the study at https://mhealth.jmir.org/2020/8/e19857
Patient travel history can be crucial in evaluating evolving infectious disease events. Such information can be challenging to acquire in electronic health records, as it is often available only in unstructured text.
Objective: This study aims to assess the feasibility of annotating and automatically extracting travel history mentions from unstructured clinical documents in the Department of Veterans Affairs across disparate health care facilities and among millions of patients. Information about travel exposure augments existing surveillance applications for increased preparedness in responding quickly to public health threats.
Methods: Clinical documents related to arboviral disease were annotated following selection using a semiautomated bootstrapping process. Using annotated instances as training data, models were developed to extract from unstructured clinical text any mention of affirmed travel locations outside of the continental United States. Automated text processing models were evaluated, involving machine learning and neural language models for extraction accuracy.
Results: Among 4584 annotated instances, 2659 (58%) contained an affirmed mention of travel history, while 347 (7.6%) were negated. Interannotator agreement resulted in a document-level Cohen kappa of 0.776. Automated text processing accuracy (F1 85.6, 95% CI 82.5-87.9) and computational burden were acceptable such that the system can provide a rapid screen for public health events.
Conclusions: Automated extraction of patient travel history from clinical documents is feasible for enhanced passive surveillance public health systems.
Without such a system, it would usually be necessary to manually review charts to identify recent travel or lack of travel, use an electronic health record that enforces travel history documentation, or ignore this potential source of information altogether. The development of this tool was initially motivated by emergent arboviral diseases. More recently, this system was used in the early phases of response to COVID-19 in the United States, although its utility was limited to a relatively brief window due to the rapid domestic spread of the virus. Such systems may aid future efforts to prevent and contain the spread of infectious diseases. read the study at https://publichealth.jmir.org/2021/3/e26719
|
|
Scooped by
nrip
|
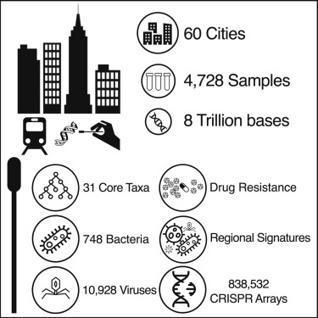
Here is a global atlas of 4,728 metagenomic samples from mass-transit systems in 60 cities over 3 years, representing the first systematic, worldwide catalog of the urban microbial ecosystem. This atlas provides an annotated, geospatial profile of microbial strains, functional characteristics, antimicrobial resistance (AMR) markers, and genetic elements, including 10,928 viruses, 1,302 bacteria, 2 archaea, and 838,532 CRISPR arrays not found in reference databases. Authors identified 4,246 known species of urban microorganisms and a consistent set of 31 species found in 97% of samples that were distinct from human commensal organisms. Profiles of AMR genes varied widely in type and density across cities. Cities showed distinct microbial taxonomic signatures that were driven by climate and geographic differences. These results constitute a high-resolution global metagenomic atlas that enables discovery of organisms and genes, highlights potential public health and forensic applications, and provides a culture-independent view of AMR burden in cities.
|
|
Scooped by
nrip
|
Background: In March 2020, South Africa implemented strict nonpharmaceutical interventions (NPIs) to contain the spread of COVID-19. Over the subsequent 5 months, NPI policies were eased in stages according to a national strategy. COVID-19 spread throughout the country heterogeneously; the case numbers peaked from July to August. A second COVID-19 wave began in late 2020. Data on the impact of NPI policies on social and economic well-being and access to health care are limited.
Objective: We aimed to determine how rural residents in three South African provinces changed their behaviors during the first COVID-19 epidemic wave.
Methods: The South African Population Research Infrastructure Network nodes in the Mpumalanga (Agincourt), KwaZulu-Natal, (Africa Health Research Institute) and Limpopo (Dikgale-Mamabolo-Mothiba) provinces conducted up to 14 rounds of longitudinal telephone surveys among randomly sampled households from rural and periurban surveillance populations every 2-3 weeks. Interviews included questions on the following topics: COVID-19–related knowledge and behaviors, the health and economic impacts of NPIs, and mental health. We analyzed how responses varied based on NPI stringency and household sociodemographics.
Conclusions: South Africans complied with stringent, COVID-19–related NPIs despite the threat of substantial social, economic, and health repercussions. Government-supported social welfare programs appeared to buffer interruptions in income and health care access during local outbreaks. Epidemic control policies must be balanced against the broader well-being of people in resource-limited settings and designed with parallel support systems when such policies threaten peoples’ income and access to basic services.
|
|
Scooped by
nrip
|
The major medical and social challenge of the 21st century is COVID-19, caused by the novel coronavirus SARS-CoV-2. Critical issues include the rate at which the coronavirus spreads and the effect of quarantine measures and population vaccination on this rate. Knowledge of the laws of the spread of COVID-19 will enable assessment of the effectiveness and reasonableness of the quarantine measures used, as well as determination of the necessary level of vaccination needed to overcome this crisis. Objective: This study aims to establish the laws of the spread of COVID-19 and to use them to develop a mathematical model to predict changes in the number of active cases over time, possible human losses, and the rate of recovery of patients, to make informed decisions about the number of necessary beds in hospitals, the introduction and type of quarantine measures, and the required threshold of vaccination of the population. Methods: This study analyzed the onset of COVID-19 spread in countries such as China, Italy, Spain, the United States, the United Kingdom, Japan, France, and Germany based on publicly available statistical data. The change in the number of COVID-19 cases, deaths, and recovered persons over time was examined, considering the possible introduction of quarantine measures and isolation of infected people in these countries. Based on the data, the virus transmissibility and the average duration of the disease at different stages were evaluated, and a model based on the principle of recursion was developed. Its key features are the separation of active (nonisolated) infected persons into a distinct category and the prediction of their number based on the average duration of the disease in the inactive phase and the concentration of these persons in the population in the preceding days. Results: Specific values for SARS-CoV-2 transmissibility and COVID-19 duration were estimated for different countries. In China, the viral transmissibility was 3.12 before quarantine measures were implemented and 0.36 after these measures were lifted. For the other countries, the viral transmissibility was 2.28-2.76 initially, and it then decreased to 0.87-1.29 as a result of quarantine measures. Therefore, it can be expected that the spread of SARS-CoV-2 will be suppressed if 56%-64% of the total population becomes vaccinated or survives COVID-19. Conclusions: The quarantine measures adopted in most countries are too weak compared to those previously used in China. Therefore, it is not expected that the spread of COVID-19 will stop and the disease will cease to exist naturally or owing to quarantine measures. Active vaccination of the population is needed to prevent the spread of COVID-19. Furthermore, the required specific percentage of vaccinated individuals depends on the magnitude of viral transmissibility, which can be evaluated using the proposed model and statistical data for the country of interest. read the entire paper at https://publichealth.jmir.org/2021/4/e21468/
|
|
Scooped by
nrip
|
When it comes to loosening COVID restrictions all eyes are usually trained on the famous R number. But as epidemiologists Julia Gog and Thomas House recently explained to us, there's also another important factor to consider alongside R. That's the prevalence of COVID-19 in the population: the proportion of people who currently have the disease. Put simply, if prevalence has been so high that the NHS is in crisis, then opening up might stretch it to breaking point, even if R is less than 1, or would remain so. If, on the other hand, prevalence is very low, we might be able to tolerate a higher value of R as it would not immediately lead to many cases. This is true particularly if prevalence has been low for some time. We've illustrated this idea in the schematic plot below. The vertical axis measures prevalence and the horizontal axis measures R. Any point on this plot, such as the one we marked in black right in the middle, corresponds to a situation where we have the value of R that lies directly beneath the point on the horizontal axis, and the value of prevalence that lies directly to the left of the point on the vertical axis read this excellent piece at https://plus.maths.org/content/R-not-all?nl=0
|
|
Scooped by
nrip
|
The WHO Hub for Pandemic and Epidemic Intelligence will be a global platform for pandemic and epidemic intelligence, creating shared and networked access to vital multi-sectoral data, driving innovations in data analytics and building the communities
of practice needed to predict, prevent, detect, prepare for and respond to worldwide health threats. The WHO Hub will be a new global collaboration of countries and partners worldwide, driving innovations to increase availability and linkage of diverse data; develop tools and predictive models for risk analysis; and to monitor disease control measures
and infodemics. The WHO Hub will enable partners from around the world to collaborate and co-create the tools and data access that all countries need to prepare, detect and respond to pandemic and epidemic risks. The World Health Organization (WHO) and the Federal Republic of Germany will establish a new global hub for pandemic and epidemic intelligence, data, surveillance and analytics innovation. The Hub, based in Berlin and working with partners around the
world, will lead innovations in data analytics across the largest network of global data to predict, prevent, detect prepare for and respond to pandemic and epidemic risks worldwide. Critically, the WHO Hub will support the work of public health experts and policy-makers in all countries with insights so
they can take rapid decisions to prevent and respond to future public health emergencies.“We need to identify pandemic and epidemic risks as quickly as possible, wherever they occur in the world. For that aim, we need to strengthen the global early warning surveillance system with improved collection of health-related data and inter-disciplinary risk analysis,” said Jens Spahn, German Minister of Health. Working with partners globally, the WHO Hub will drive a scale-up in innovation for existing forecasting and early warning capacities in WHO and Member States. At the same time, the WHO Hub will accelerate global collaborations across public and private sector organizations, academia, and international partner networks. It will help them to collaborate and co-create the necessary tools for managing and analyzing data for early warning surveillance. It will also promote greater access to data and information. “One of the lessons of COVID-19 is that world needs a significant leap forward in data analysis to help leaders make informed public health decisions,” said Dr Tedros Adhanom Ghebreyesus, WHO Director-General. “This requires harnessing the potential of advanced technologies such as artificial intelligence, combining diverse data sources, and collaborating across multiple disciplines. Better data and better analytics will lead to better decisions.” read the release at the WHO website at https://www.who.int/news/item/05-05-2021-who-germany-launch-new-global-hub-for-pandemic-and-epidemic-intelligence also useful to read the note on the UN website about the same https://news.un.org/en/story/2021/05/1091332
|
|
Scooped by
nrip
|
Communicable diseases including COVID-19 pose a major threat to public health worldwide. To curb the spread of communicable diseases effectively, timely surveillance and prediction of the risk of pandemics are essential. The aim of this study is to analyze free and publicly available data to construct useful travel data records for network statistics other than common descriptive statistics. This study describes analytical findings of time-series plots and spatial-temporal maps to illustrate or visualize pandemic connectedness. We observed similar patterns in the time-series plots of worldwide daily flights from January to early-March of 2019 and 2020. A sharp reduction in the number of daily flights recorded in mid-March 2020 was likely related to large-scale air travel restrictions owing to the COVID-19 pandemic. The levels of connectedness between places are strong indicators of the risk of a pandemic. Since the initial reports of COVID-19 cases worldwide, a high network density and reciprocity in early-March 2020 served as early signals of the COVID-19 pandemic and were associated with the rapid increase in COVID-19 cases in mid-March 2020. The spatial-temporal map of connectedness in Europe on March 13, 2020, shows the highest level of connectedness among European countries, which reflected severe outbreaks of COVID-19 in late March and early April of 2020. The analysis can facilitate early recognition of the risk of a current communicable disease pandemic and newly emerging communicable diseases in the future. read the study at https://publichealth.jmir.org/2021/3/e27317
|
|
Scooped by
nrip
|
National governments worldwide have implemented non-pharmaceutical interventions to control the COVID-19 pandemic and mitigate its effects.
Objective: The aim of this study was to investigate the prediction of future daily national confirmed COVID-19 infection growth—the percentage change in total cumulative cases—across 14 days for 114 countries using non-pharmaceutical intervention metrics and cultural dimension metrics, which are indicative of specific national socio-cultural norms.
Methods: We combined the Oxford COVID-19 Government Response Tracker data set, Hofstede cultural dimensions, and daily reported COVID-19 infection case numbers to train and evaluate five non–time series machine learning models in predicting confirmed infection growth.
We used three validation methods—in-distribution, out-of-distribution, and country-based cross-validation—for the evaluation, each of which was applicable to a different use case of the models.
Results: Our results demonstrate high R2 values between the labels and predictions for the in-distribution method (0.959) and moderate R2 values for the out-of-distribution and country-based cross-validation methods (0.513 and 0.574, respectively) using random forest and adaptive boosting (AdaBoost) regression.
Although these models may be used to predict confirmed infection growth, the differing accuracies obtained from the three tasks suggest a strong influence of the use case.
Conclusions: This study adds to the rapidly growing body of work related to predicting COVID-19 infection rates by introducing an approach that incorporates routinely available data on NPIs and cultural dimensions. Importantly, this study emphasizes the utility of NPIs and cultural dimensions for predicting country-level growth of confirmed infections of COVID-19, which to date have been limited in existing forecasting models. Our findings offer a new direction for the broader inclusion of these types of measures, which are also relevant for other infectious diseases, using non–time series machine learning models. Our experiments also provide insight into validation methods for different applications of the models.
read the entire study at https://www.jmir.org/2021/4/e26628
|